West Nile Virus
WNV
Profile
West Nile fever is caused by the West Nile virus (WNV). The virus is transmitted by gnats (mosquitoes of the genus Culex), and birds (over 300 bird species) act as the natural reservoir. Humans and other mammals, especially horses, can also become ill. However, humans and horses represent a dead end for the virus - they can become ill but cannot transmit the virus to other mosquitoes. Thus, the virus cannot be transmitted from horse to horse, nor from horse to human.
Occurrence
The West Nile virus is endemic in various regions, including Africa, Israel, western Turkey, the Middle East, India, and North and Central America. In Europe, isolated cases as well as seasonal outbreaks are reported every year from countries in southern, eastern and western Europe. In Europe, the West Nile virus is mainly transmitted by ‘native’ mosquito species.
The website of the European Centre for Disease Prevention and Control (ECDC) provides an overview of the geographical distribution of reported West Nile virus infections in humans and animals – ECDC – WNV Dashboard
For reports of West Nile virus infections in animals, see Situation in Europe
Pathogen reservoir
The natural reservoir of West Nile virus is birds, in particular migratory birds (especially Passeriformes such as corvids and sparrows), and it can be spread over long distances via these birds. Birds of prey such as hawks and falcons also contract West Nile Virus and are often indicator animals for virus presence in Central Europe.
Furthermore, various mammals (monkeys, horses, cattle, goats, sheep, deer, buffalo, camelids, pigs, dogs, wolves, foxes, bears, cats, bats, skunks, squirrels, hares and other rodents), reptiles (alligators, snakes), amphibians as well as humans can be infected. Mammals, reptiles and amphibians do not play a significant role in the further spread of the virus as final hosts.
To date, there have been no reports of West Nile virus infections in humans or animals in Austria for the year 2026 (as at 29 July 2026).
In 2025, there were three reported cases of West Nile virus infection in animals and one imported case in humans (as at 31 December 2025).
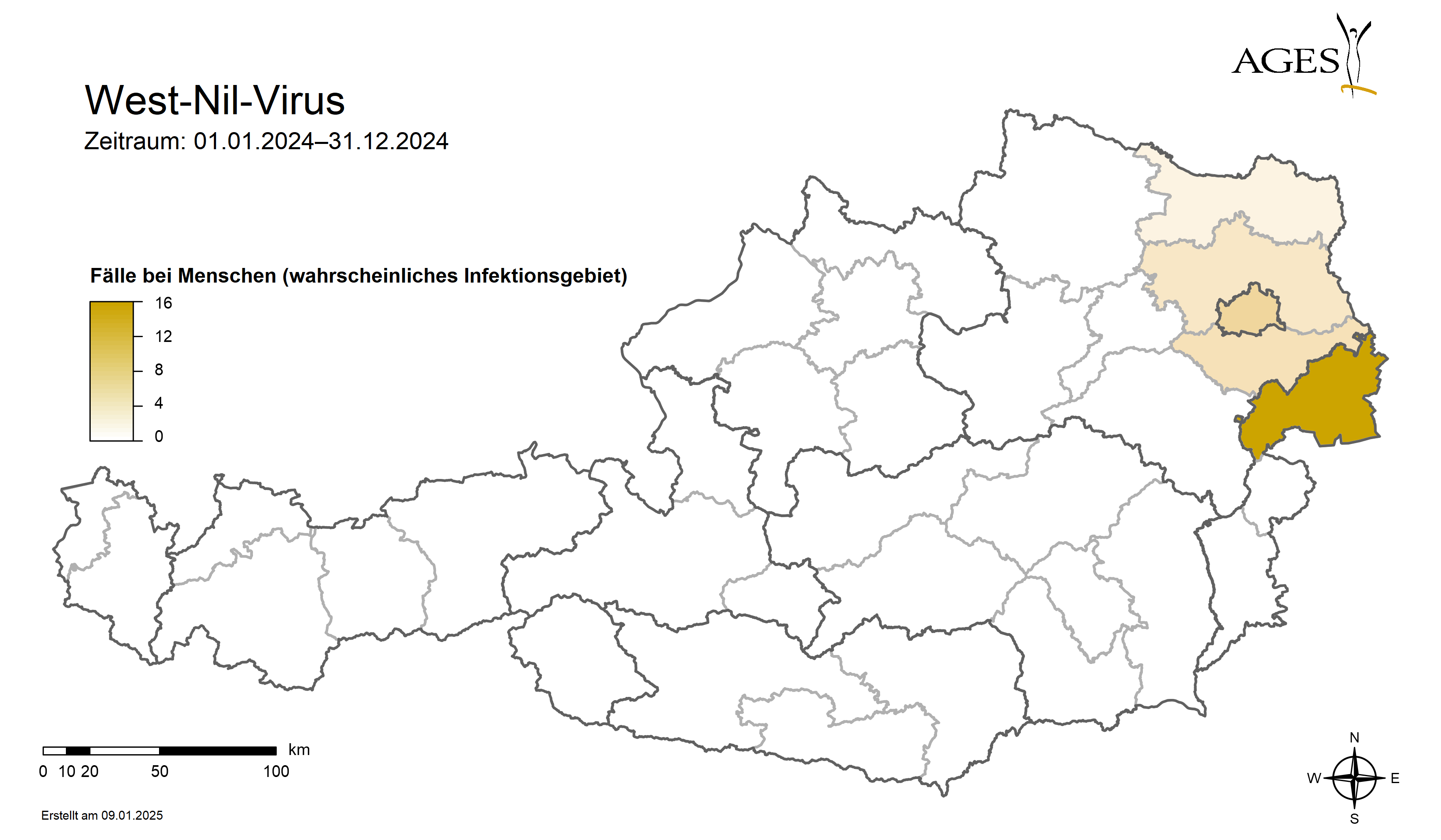
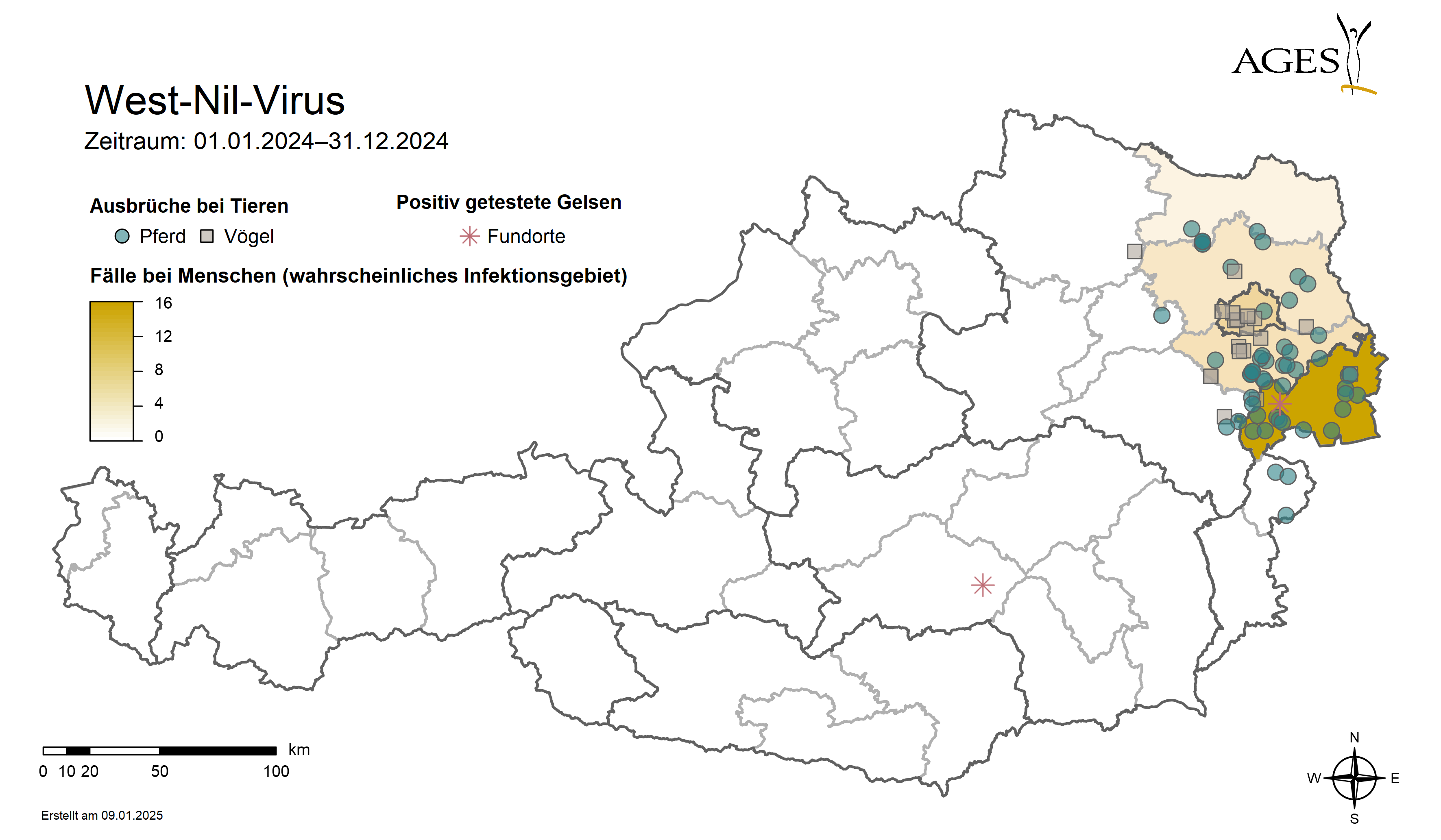
In 2024, there were more West Nile virus infections in humans and animals than in previous years. The first cases in animals occurred two months earlier than in previous years. As part of a surveillance programme, mosquitoes were also tested for the West Nile virus.
Specialist information for human medicine
The causative agent of West Nile fever is the West Nile virus (WNV). WNV is an enveloped RNA virus that is transmitted from infected birds to humans and mammals via mosquito bites of the genus Culex. Both humans and horses are dead-end hosts for the virus - they therefore act as final hosts and can contract the disease but cannot transmit the virus to other mosquitoes. The WNV strains are divided into subtypes 1 (WNV-1) and 2 (WNV-2).
A large number of different mosquito species are possible vectors, especially the genera Culex, Aedes and Ochlerotatus. In the genus Culex, these are mainly Culex quinquefasciatus, C. molestus, C. pipiens, C. restuans, C. salinarius and C. tarsalis. Culex pipiens, as a parasite of birds and humans, is one of the possible vectors in the transmission chain from animals to humans or birds to mammals. The virus can survive the winter in the mosquito Culex and undergo a reproduction cycle in the mosquito the following year in spring. After 10-15 days of incubation in the mosquito, the WNV is passed on by biting. The virus is also transmitted via direct contact. The significance of oral or faecal transmission is still unknown; ingestion of the virus via aerosols is also under discussion.
Symptoms
80 % of infections are asymptomatic. 20 % of infected patients show flu-like symptoms with sudden, high fever (= mild West Nile fever), muscle aches, headaches, gastrointestinal symptoms, possibly cold symptoms, swelling of the lymph nodes and skin spots. The incubation period is 2-8 days. The main symptoms usually subside within 7-10 days.
In individual cases (0.7 %), West Nile meningitis or encephalitis occurs. Neuroinvasive disorders with clouding of consciousness, coordination disorders, difficulty swallowing, extreme tiredness and dizziness combined with behavioural and personality changes are typical signs. Hepatitis, myocarditis, nephritis, pancreatitis and splenomegaly coupled with a long convalescence are the result. Immunocompromised patients and people over the age of 50 have a higher risk of developing the severe form of the disease.
In 2014, West Nile virus was diagnosed for the first time in a blood donor in Austria. Eight further cases were found in 2015, including five blood donors. Human-to-human transmission is extremely rare, but transmission through blood transfusion, organ transplantation, intrauterine exposure and/or breastfeeding is possible.
The risk of contracting West Nile fever in Austria is currently still very low. As the virus is transmitted by mosquitoes, West Nile virus infections occur in the summer months. A total of 55 domestically acquired West Nile virus cases were confirmed in Austria between 2010 and 2022. The most likely places of infection are in Vienna, Lower Austria and Burgenland. One positive human case was reported in 2023. This was a case imported from Italy. There have been no human deaths in Austria to date.
Human diagnostics
National Reference Centre for Flavivirus Infections in Humans
Department of Virology, Medical University of Vienna
Kinderspitalgasse 15, 1095 Vienna
Tel: +43 1 40 160 65517
Specialist information for veterinary medicine
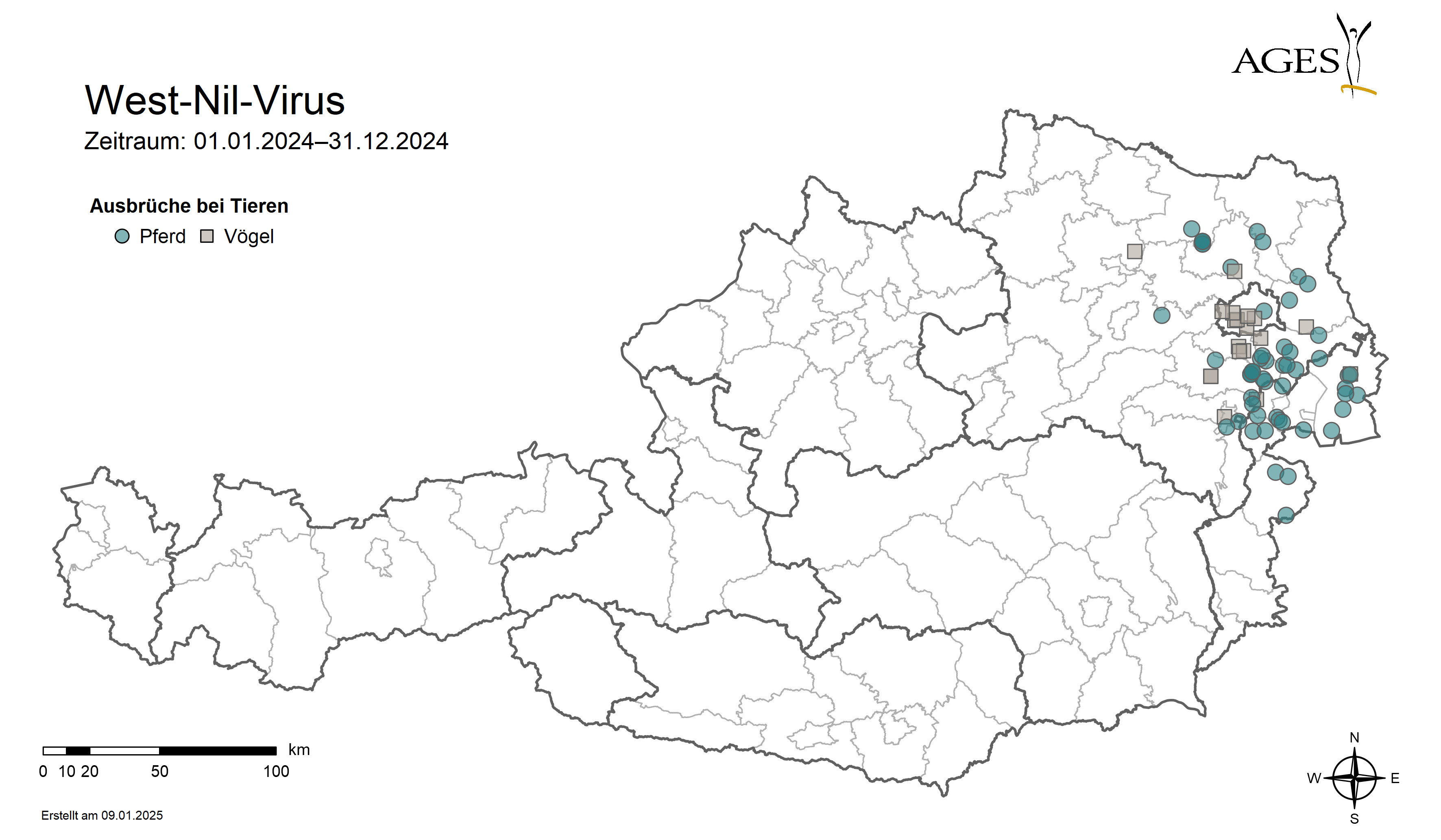
In animals, clinical WNV infections in birds of prey were first detected in Austria in 2008. Since then, WNV-2 cases have continued to be detected sporadically in birds of prey(Falconiformes), passerines(Passeriformes) and corvids(Corvidae, ravens and crows), which play a central role in the spread of the pathogen, as part of a surveillance programme. A surveillance programme for WNV-specific antibodies in horses has been running throughout Germany since 2011.
The first clinical WNV infections in horses were first detected in Austria in summer 2016. Further cases then occurred in the years 2017 to 2020 and 2023 to 2024.
In Austria, WNV activity in 2024 was earlier and more intense than in previous years. The first detection in 2024 occurred almost two months earlier than in 2023 (at the end of September 2023 in an eagle owl in Vienna). At the end of July, WNV-2 was detected in a Hooded Crow from Burgenland (Eisenstadt-Umgebung district). Increased infections in humans and animals have been reported, particularly in eastern Austria (Vienna, Lower Austria, Burgenland). Given the favourable weather conditions for the transmission of WNV in the EU, further cases were detected in horses and birds in the months from August to November 2024. The last case in horses was reported in mid-November 2024.
Information on West Nile fever cases in animals is available in the monthly animal disease radar.
AGES mosquito monitoring for the surveillance of vectors (carriers) of human pathogenic viruses such as West Nile virus is used to collect and classify mosquitoes at predefined locations. Molecular biological methods are used to specifically determine the infestation rate of mosquito populations with West Nile virus and other pathogens.
Symptoms in birds
Birds usually show few or no clinical symptoms; CNS symptoms with corresponding accompanying symptoms may be diagnosed: Lethargy, coordination difficulties, ataxia, depression, torticollis, opisthotonos and haemorrhages in the beak and cloacal region. Young birds (1-11 day old chicken chicks, goslings) show a much more pronounced viraemia than older birds. A high mortality rate is found in crows and other corvids. Myocarditis and encephalitis are frequently diagnosed in dead birds. Experimentally infected chickens and turkeys showed no symptoms. Symptoms in geese were loss of appetite, weight loss, depressive behaviour, myocarditis and neurological disorders. Rhythmic sideways head movements ("sideways oscillation") were frequently observed.
Symptoms in mammals
Horses have a higher risk of infection than humans, so in an affected area clinical disease usually occurs earlier in horses. The disease is asymptomatic in 90% of cases. The clinical signs in horses are often non-specific and similar to those of other diseases, especially CNS diseases. Common symptoms include fever, mild ataxia, depression or lethargy, propping of the head, weakness of the hindquarters, generalised muscle weakness, loss of appetite, visual disturbances, partial paralysis, convulsions and coma. In clinically ill horses, the infection is lethal in up to 40 % of animals.
In dogs and cats, the course of the disease is usually asymptomatic. There are no known cases of direct dog or cat-human transmission.
In sheep, neurological disorders, ataxia, fever and behavioural disorders (teeth grinding, depression) occur. In ewes, abortion or stillbirth can occur. Death can also occur in young lambs shortly after birth. Infected ewes can die.
Therapy and prophylaxis
Specific treatment of a WNV infection is currently not possible. Clinically infected horses require general intensive medical care with symptomatic therapy.
Vaccines against West Nile virus for horses have been approved in Austria for prophylaxis since 2011. Basic immunisation consists of two vaccinations three to five weeks apart, after which annual booster vaccinations are required. Protection against infection is only available two to three weeks after the second vaccination at the earliest.
In addition to international competition horses, leisure horses should also be adequately protected against this dangerous disease - very simple measures are often sufficient:
- Bringing the horses into the stable at certain times when the insects are particularly active (dawn and dusk).
- Use of mosquito repellents on the animals themselves, which are suitable for horses and commercially available on the market
- Installing mosquito screens and insect repellent lamps in the stable
Mosquito breeding sites such as standing water on the property should be avoided. Standing shallow puddles, such as those often found in used tyres, near manure heaps or drainage systems, are ideal breeding grounds for all types of mosquitoes.
If possible, birds should not be able to fly into a horse stable or chickens should not be kept in the same stable room, as they can also be a source of infection.
Veterinary diagnostics
Clinical WNV encephalitis is confirmed using direct and indirect detection methods. Suitable sample materials are
- Serum (IgG and IgM ELISA, SNT)
- Urine (RT-PCR)
- CSF (RT-PCR)
- Organ material (incl. CNS)
Indirect detection of a WNV infection from serum:
An immunoglobulin G (IgG) ELISA, which detects antibodies against flaviviruses, and a WNV-IgG specific ELISA test are used for the examination of horse sera. A WNV-IgM Elisa is used to detect acute antibodies, and a specific WNV serum neutralisation test is performed for an exact titer determination of antibodies against WNV.
If antibodies are found, it must be ensured that they are not vaccine antibodies (proof of vaccination of the horse, WNV antibody titre increase in paired serum samples) or whether the tested animal has spent time in endangered areas abroad (competition sport) before the test. Only in this way can an autochthonous infection of horses in Austria be ruled out or confirmed with a high degree of certainty.
Virus detection of a WNV infection in fatal or progressive cases of WNV encephalitis is confirmed not only by neuropathohistological examination but also by direct detection methods (real-time RT-PCR, sequencing, virus isolation and immunohistochemistry if necessary).
A WNV PCR test is carried out on the organ material of dead animals and, if positive, confirmed by means of additional WNV subtyping methods or sequencing of the WNV strain.
If encephalitis is clinically suspected in equidae, a WNV infection should be clarified promptly due to the AHL notification obligation (category E disease). In the case of acute disease, it is recommended that blood and urine samples be sent in. In progressive forms with an unfavourable prognosis or a fatal outcome, the CNS of the affected animals should be further examined at the National Reference Laboratory. Due to the zoonotic potential of most of the pathogens to be considered for differential diagnosis, the head should be removed and sent in (in compliance with biosecurity measures).
The most important differential diagnoses are infections with flaviviruses such as TBEV and Japanese encephalitis (JEV), infections with varicellovirus equidalpha 1 (formerly equine herpes virus 1, EHV-1) and/or varicellovirus equidalpha 4 (formerly equine herpes virus 4, EHV-4), Bornasche disease and rabies. If there are molecular biological and histopathological indications of the presence of viral American equine encephalitis (Eastern equine encephalitis virus (EEEV), Western equine encephalitis virus (WEEV) or Venezuelan equine encephalitis virus (VEEV)), the samples are forwarded to the European Reference Laboratory in France.
In birds, highly pathogenic avian influenza and Newcastle disease viruses as well as septicaemic bacterial infections should primarily be considered in the differential diagnosis.
Contact
Institut für veterinärmedizinische Untersuchungen Mödling
- vetmed.moedling@ages.at
- +43 50 555 38112
-
Robert Koch-Gasse 17
2340 Mödling
{kind=link}
{kind=link}
{kind=link}
Last updated: 30.07.2026
automatically translated